



Syamimi Shamsuddina, b*, Hanafiah Yussofb, Luthffi Idzhar Ismailb, Salina Mohamedc, Fazah Akhtar Hanapiahc and Nur Ismarrubie Zaharid
aFaculty of Manufacturing Engineering, Universiti Teknikal Malaysia Melaka, Hang Tuah Jaya, 76100 Durian Tunggal, Melaka, Malaysia.
bCOE for Humanoid Robots & Bio-sensing (HuRoBs), Fac. of Mechanical Engineering, Universiti Teknologi MARA (UiTM) Shah Alam, 40450, Malaysia
cFaculty of Medicine,Universiti Teknologi MARA (UiTM) Shah Alam, 40450, Malaysia
dDepartment of Mechanical and Manufacturing, Faculty of Engineering, Universiti Putra Malaysia, Serdang 43400, Malaysia
* Corresponding author. Syamimi Shamsuddin Tel.: +60 3 5543 5161 ; fax: +60 3 5543 5160. E-mail address: syamimi@ieee.org
Abstract: The evolution of human-robot interaction (HRI) is now expanding its wings to aid children with Autism Spectrum Disorders (ASD) in areas of socialization, communication and playful behavior through robot-based intervention. Herein we present our holistic, long- standing goal to contribute to the lives of children with ASD; who suffer a lifelong developmental disability. The purpose of this paper is to elaborate on a case study in our pilot experiment where a child with ASD is exposed to the humanoid robot NAO in order to gauge his initial response and behavior in the presence of a robot. NAO robot is the chosen robotic agent as it is a commercially available humanoid with simpler in appearance compared to real humans, thus appears more approachable to children with ASD.
The pilot procedures involve the robot executing basic, simple components of interaction through a series of 5 different modules. In this study, the principal results show that the basic HRI carried out by the robot is able to suppress the child’s autistic behavior during the child-robot interaction. Also, more eye contact is observed between the child and robot compared to the child with his teacher during regular class session.
Relating this to the child’s IQ which falls in the moderate category, it is suggested that children with ASD in the same IQ group will be receptive to robot-based intervention even in the first interaction session. Hence, it can be concluded that the humanoid robot NAO has potential to serve as a platform to support and initiate interaction in children with ASD.
Keywords: human-robot interaction (HRI); Autism Spectrum Disorders (ASD); humanoid robot NAO; rehabilitation robotics
1. Introduction
The colossal area of robotics research is no longer confined to the solitary labs in universities and learning institutions. Varying types of robots are now gaining places in our lives in a multitude of roles as robots are no more constrained to images of heavy manipulators doing repetitive tasks in the manufacturing line. The expanding role of robots coincides with the sole purpose of improving the lives of mankind.
Notably, the global population that expands every second signifies the growing number of people born with disabilities and also the prevalence of disability that increases steadily with age. As these disabled people are a part of the society that we live in, it is crucial for them to receive proper care and rehabilitation so that they can live the lives of normal people as much as possible.
Effective usage of robotics technology in aid of the disabled holds promising and effective possibilities as it is motivating, accurate, objective and adaptive to the needs of individuals. Hence, rehabilitation robotics is part of the notion for robots to play substantial role in healthcare and specific rehab interventions for the elderly people and persons affected by neurodevelopmental disorders such as Cerebral Palsy (CP) and Autism Spectrum Disorders (ASD). With robotic intervention, it is hoped that the quality of life for the disabled can be made better [1] and they may gain more independence in their daily lives.
At the Center for Humanoid Robots and Bio-sensing (HuRoBs) laboratory in Universiti Teknologi MARA (UiTM), our research motivation lies in our long-standing goal to contribute to a group of community that suffers from Autism Spectrum Disorders (ASD). Our multi-disciplinary team comprises of engineering researchers, therapists and also experienced clinicians that work together for the same purpose. We believe that by using engineering and medical knowledge, coupled with the motivation to help these people with special needs; breakthroughs can be made and achieved. We also forge collaboration with The National Autism Society of Malaysia (NASOM) which is currently the biggest organization that caters for the education and care for children with ASD in Malaysia in order to engage their students and facilities in this research.
1.1 Human-robot Interaction (HRI)
In rehabilitation robotics, an assistive robot is broadly defined as one that gives aid or support to a human user. In robot- based intervention, human-robot interaction (HRI) architecture has been identified as a new potential approach in the research on autism. HRI is simply defined as the dynamically changing relationship between humans and intelligent robots. Socially Assistive Robotics (SAR) which is a domain in HRI has a more specific scope of helping people through social interaction rather than physical contact [2, 3]. In fact, HRI is part of the evolution in SAR system that involves intervention for children with ASD [4].
However, due to the extensive variability in terms of each robot’s physical appearance, how it is utilized in clinical setting and the highly individualized character of every ASD child; varying responses has been reported. Also, most findings are still at exploratory basis and have methodological restrictions resulting with difficulty to draw firm inferences about the clinical utility of robots [5]. Based on these issues, it is clearly seen that more exploratory research is needed in human-robot interaction (HRI) approach for ASD therapy.
1.2 Autism Spectrum Disorders (ASD)
Autism Spectrum Disorders (ASD) is a collection of disabilities that share similar traits. These disabilities revolve around the ‘triad of impairments’ which are the deficits in social interaction, communication and behavioral characteristics. The behavior disorder are marked by the restricted, repetitive and stereotyped repertoire of activity and interests [6]. In 1943, Leo Kanner M.D. was the first to identify a group of children who possess characteristics of showing extreme withdrawal and disability in forming usual social relations with people [7]. He referred this condition as ‘early infantile autism’.
ASD shall manifest itself during the first three years of a child’s life. As it stems from a neuro-developmental disorder resulting with affected brain function; a person’s skills in communication and social interaction skills are duly impacted. A child with ASD oftentimes has difficulties to engage with peers as he or she lacks in social or emotional reciprocity. Each individual with ASD is unique as there are no two people with ASD who possess the same autistic characteristics. At one end of the spectrum, the children may possess apparent deficit in social and communication and be mentally handicapped. On the other end with high-functioning ASD, a child may have the ability to do math, write but unable to hold eye-contact or participate in a conversation. The whole range is also termed as Pervasive Development Disorders (PDD) [8].
With statistics estimating 1 in every 91 children in the United States [9] and 1 in every 150 children in Malaysia [10] are diagnosed with ASD, the need of suitable rehabilitation measures are crucial. Looking at the prevalence of ASD in countries all over the world, it is understandable that the need of effective intervention for ASD to be classified as public health emergency [11]. This is why for young children with ASD, the earlier they began to get help, the more opportunities will be accessible for them in the future.
As ASD is not curable and evidence based results for most therapeutic interventions are limited [12], only proper treatment and therapy shall help these children to lead normal lives and grow to be independent adults. Through intervention and rehabilitation, they can emerge and free themselves (if not entirely) from their autistic disabilities to function like a near normal child.
1.3 HRI for Children with ASD
The first and pioneering effort of using robots for autism therapy was made in 1976 by pediatrician Sylvia Weir and psychotherapist Ricky Emanuel with a mobile turtle-like robot LOGO at University of Edinburgh [13]. No other significant breakthroughs have been identified in similar context until the late 1990s. As autism prevalence rate continues to escalate, more research labs have also started to explore the possibilities of employing robots to be a part of the therapy for children with ASD. These children have been known to be attracted to inanimate, technological objects namely computers, gadgets and robots. On the other hand, the robot itself is much simpler in appearance compared to real life objects, its behavior can be custom-made to suit different scenarios and it has the capacity to offer expected and simpler interaction with the children. These two complementing factors make robots the ideal medium to be used in autism therapy.
Due to the unlimited potential of robot-based therapy for people challenged with ASD, this method continues to be adopted to scaffold social skills [14, 15], communication skills [4, 16], promoting explorative behavior [17] and early diagnosis [11, 18] amongst children with autism. In recognition of these promising possibilities of robot-based intervention, human-robot interaction (HRI) architecture has great potential to teach children with ASD how to detect and understand emotions and social behaviors [19]. In fact, robots can provoke interactive and social responses that are not naturally occurring in children with ASD [20]. It also can reduce cost since the robot can easily be reprogrammed according to the ASD criteria.
Associated with their deficit in social and communication skills, ASD children are oftentimes subjected to depression and anxiety when interacting with fellow peers due to the unpredictability and complexity of human behaviors. On the other hand, ordinary toys are unable to prompt responses and engage in play scenarios with the ASD children. Hence, the controllable autonomy of robots offers the best of both worlds [15] and resulting with the robots as propitious social partners for these disabled children.
2. The robot and experiment protocols
2.1 Humanoid robot NAO and justification for a robot in human form
The evolution of robots has always been a fascinating subject for both generalists and technologists alike. A robot is defined as ‘an autonomous system which exists in the physical world, can sense its environment, and can act on it to achieve some goals’ [21]. Humanoids, robots in human form, pose even greater interest to men as they are regarded as the future of robotics [22]. Sociable humanoid robots have become the catalyst as to how the world perceives machines.
Review of past studies has identified HRI as part of the intervention for children with ASD. Nevertheless, most explored robotic systems in the earlier works are mainly in the form of toys, not humanoid-form social partners [13]. As human-like robots pose greater potential in ASD therapy for skills generalization [23], the application of intelligent robotic system in the form of humanoid begun to gain its momentum. At the University of Texas at Arlington, an emotional humanoid robot with expressive skin called Zeno [24] is studied for its potential to aid ASD subjects to undergo therapy in a realistic and engaging manner. The minimally expressive humanoid robot KASPAR that has been shown to be an important object in encouraging interaction in children with ASD [25] and Robota, a humanoid robotic doll that encourages human-human interaction [26] are past studies that explores the usage of robots in human form as part of ASD therapy.
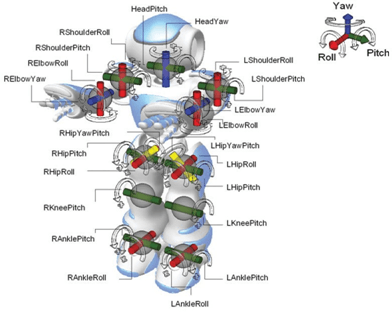
With the introduction of humanoid robot NAO by Aldebaran-Robotics in 2008, a performant biped robot is now available and affordable for research laboratories and the mass market [27]. This humanoid robot had been designed purposely to look approachable and portray emotions like a toddler. Figure 1 shows the overall appearance of the robot.
 |
 |
Fig. 1. The humanoid robot NAO by Aldebaran Robotics in France
The birth of NAO shed greater light in robotic intervention for children with disabilities. It’s predictable and repetitive behaviors may be able to train children with ASD on how to understand and perceive human emotions, a skill in human interaction that they are lacking. In the light of ASD intervention, current research avenues involving NAO are being carried out at Eindhoven University for social skill training [28], at ENSTA ParisTech to train postural expressions [29], at University of Connecticut to increase sociability [30], at University of Notre Dame to create understanding of gestures and facial expression and at Vanderbilt University for ASD diagnosis [11].
The rationalization of using a robot in human form is due to the fact that in appearance-wise, a humanoid’s body structure is similar to an actual human. Therefore, a humanoid is suitable to engage the children with ASD in imitation- based therapy and therapies that promote joint attention. As suggested in [23], utilization of a robot in human form pave ways to more possibilities in teaching skills generalization to children with ASD.
The humanoid robot NAO by Aldebaran is also commercially available and simpler in appearance compared to real humans, thus seems more approachable to these children. Plus, NAO is built in the size of a two-year old child. This fits the requirements of robot design for autism therapy that requires the robot’s size to roughly be the size of a human toddler [31].
2.2 The experiment: pilot set-up and modules of interaction
The pilot experiment is carried out at a NASOM center that caters specifically for children and youths with ASD. This is also where the samples of ASD children are obtained. During the child-robot interaction, each child will be accompanied by his or her class teacher. The role of the teacher is not to give any instructions to the child but only act as a ‘comforting presence’ to the child with ASD as the pilot experiment exposes the humanoid robot NAO for the first time to the child.
The experimental procedure is designed to serve as a platform in fundamental investigation of HRI and humanoid robot in the therapy of children with ASD. The pilot procedure involves the robot executing its pre-programmed behaviors in an autonomous mode. A total of 5 modules are executed by NAO to entice reaction and interaction from the ASD children. The content of each module is decided based upon discussion with experienced clinicians in ASD therapy and intensive review studies.
When the robot is executing the modules, initial response and behavior of the ASD child are recorded. During the recording, the manual operator will not be visible to the children. The operator will be monitoring the video stream from the 2 external cameras. Throughout every module in the experiment, the interaction between a child and humanoid robot NAO will be supervised by the child’s teacher. The total duration of the 5 modules are 14 minutes and 30 seconds; excluding the 30-seconds break in between the modules. Detailed explanations on the experimental set-up has been presented in [32].
The modules are listed below:
- Module 1: Introductory Rapport
- Module 2: NAO Talks
- Module 3: NAO Arm Movement
- Module 4: NAO Song Play and Eyes Blink
- Module 5: NAO Song Play and Arm Movement
Each child will experience the 5 modules only once, beginning with the simplest one. The average duration of 2.9 minutes for each module is considered to be justified as the children with ASD are known not to be able to sustain interaction or interest for longer periods of time. Another aspect that we have taken into consideration is the "Conditions to Abort Procedures". These conditions include situations where:-
- The child becomes restless and uncooperative
- The child’s teacher were to request such action to abort the interaction
As a comparison, the same child is also observed in class during normal school hours for the same duration of 14 minutes and 30 seconds. This procedure is done to study his normal behavior amongst his fellow classmates in the presence of his teacher and without the presence of the robot. Thus, a comparison can be made whether the presence of a robot executing simple HRI modules will elicit or dampen the autistic characteristics of the child with ASD.
2.3 The child with ASD
The subject in this study is a boy K who is ten years old. Prior to the child-robot pilot study, K needs to undergo the IQ and diagnostic test first. This is because our team had discovered that there is an obvious dearth in previous studies that relates the subject’s IQ level and diagnosis with the children with ASD’s responses to robotic exposure.
Our early hypothesis is that the humanoid robot NAO has the capacity to lessen the child’s autistic behavior during child- robot interaction and that there is a connection that links a child’s responses to HRI interaction with his or her IQ scores. The procedure to determine the child’s IQ is carried out using the Stanford-Binet Intelligence Scale, Fifth Edition (SB5) standard intelligence test while the diagnose test utilizes the ADOS (Autism Diagnostic Observation Schedule) which is the gold standard in diagnostic evaluations for autism.
K has a non-verbal IQ score of 104 (average), verbal IQ score of 110 (high average), full-scale IQ of 107 (average) and he is diagnosed as Autism Spectrum. Although not mentioned in the DSM-IV-TR (Diagnostic and Statistical Manual of Mental Disorders: Fourth Edition-Text Revision), K can be classified as having high-functioning autism [33] as his IQ falls in the average to above-average range. The SB5 and ADOS tests had been carried out by certified psychologists who are trained to carry out the evaluation.
To participate in this pilot study, K also complies with all the exclusion criteria including no hearing and vision deficit, no abnormal eye movement, obtained his parent/guardian’s consent, able to speak and follow simple commands in English and does not possess self-injury of aggressive behavior.
3. Case Study Assessment and Evaluation
The comprehensive evaluation on the initial response of the child during our pilot study is demonstrated in the remainder of this paper using case study evaluation approach.
3.1 Behavior score sheet based on Gilliam Autism Rating Scale-Second Edition (GARS-2)
To assess the child’s scores in terms of his autistic traits, our team utilizes a behavior score sheet that is based on the Gilliam Autism Rating Scale-Second Edition (GARS-2). The GARS-2 is an autism screening tool developed to assist teachers, parents and other people who observe children to identify and diagnose autism [34]. It is a 42-questions form for individuals of ages 3 to 22 years old and divided into 3 subscales which address the definition of autism as stated in the DSM-IV-TR (Diagnostic and Statistical Manual of Mental Disorders: Fourth Edition-Text Revision) and the Autism Society of America. Subscale 1 is stereotyped behavior, subscale 2 is social interaction and subscale 3 is communication.
For observation purposes in this pilot study, only 24 items will be adopted for evaluation considering the suitability of the items in our HRI procedures. The scores for the subject K according to each subscale are presented below:
3.2 Observation Subscale 1: Stereotyped Behavior
According to DSM-IV Criteria for Autism [6], this subscale is manifested by the restricted, repetitive and stereotyped patterns of behavior, interests and activities. In our assessment sheet, 8 items are used to evaluate the stereotyped behavior shown by K.
K had shown a 2.5% of stereotyped behavior during the single session of robot interaction compared to 25% when he is observed during an actual class session. This means that for this particular subscale, his autistic behavior has become less evident during the pilot experiment of HRI. Although K looks a little bit apprehensive at the beginning of Module 1, this is probably due to fact that no prior instructions were given to him.
The justification is that we would like that all responses shown by the child to be purely natural and spontaneous; that would portray the real initial response in child-robot interaction. Based on eye contact observation, K noticeably looks at the robot repetitively; particularly when the robot’s eyes are randomly changing colors, when the robot is speaking and executing arm movements.

Fig. 2. Child K is observed to look and give attention to the humanoid robot NAO repetitively throughout the child-robot interaction; specifically when NAO is blinking its eyes randomly, talking and executing arm movements
3.3 Observation Subscale 2: Communication
The subscale of impairments in communication for child K is assessed using 10 items of assessment. For the observations, K obtained 29.8% in the deficit of communication skills during the robotic exposure compared to 70% in class. Again, this signifies that HRI is able to lessen the observed autistic characteristics to less than half of K’s actual behavior in class in terms of communication skills.
During the child-robot interaction, K only exhibited autistic traits of speaking with a flat tone with the robot and repetitively babbling unintelligible words from Module 1 to 4. In contrast to the class observation, he displayed 7 out of the 10 assessed criteria for the communication sub-scale, hence the score of 70%.
3.4 Observation Sub-scale 3: Social Interaction
The third sub-scale addresses the deficit in social interaction, which evaluates the child’s ability to relate appropriately to people, events and objects [34]. A total of 6 six items assess this sub-scale in our behavior score sheet and K had displayed a 10% rating in this sub-scale during child-robot interaction, compared to 16.7% during his observation in class. Though the same pattern of lower score during robot interaction is observed but there is not much difference with his scores for the class observation.
Nonetheless, it is observed from the video recordings that K noticeably avoids eye contact with his teacher during conversation and when she is looking at him during the class session.
4. Results and Discussion
The goal of this study is to gauge whether the autistic characteristics of K, a child diagnosed with ASD; will become less evident (based on his behavior scores) during robotic exposure compared to normal environment in class. For child K, it is noted that he is able to focus on the robot repetitively, even if only when the robot is randomly changing its eye colors, talking and executing arm movements. The comparison of scores between these two set-ups are carried out in three sub-scales namely stereotyped behavior, communication and social interaction are shown in Figure 3 below. The figure shows that the single session of HRI exposure to K is able to dampen his autistic traits compared to his normal behavior in classroom. It is also observed that more eye contact is observed between the child and robot compared to the child with his teacher during regular class session.
As a whole, these observations suggest that NAO’s simple appearance compared to actual humans is able to act as a pull- factor to ignite the child’s interest to sustain interaction. Furthermore, NAO’s capability to have multihued eye colors, talk and play music adds up to make it a promising platform in teaching the children with ASD to initiate joint attention with the robot which later on would expand to include fellow peers and people around them.
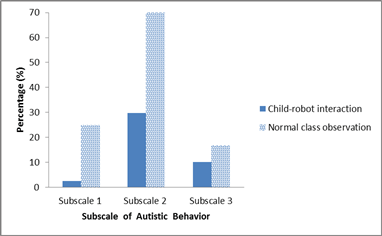 Fig. 3. The graph shows the comparison of scores (in percentage) that indicate the autistic behavior shown by child K
Fig. 3. The graph shows the comparison of scores (in percentage) that indicate the autistic behavior shown by child K
5. Conclusion
This paper reports and discusses the results from a pilot study involving a ten-year-old child with ASD to observe his autistic traits in two different settings: during HRI and regular class session. In the case of the robot acting as an object to attract attention, various research groups have carried out clinical studies to promote joint attention in children with ASD using robots. Because difficulties in sustaining joint attention are one of the manifestations of autism; helping the children with ASD to focus and give attention is critical to help them in learning and also acknowledge the presence of other people around them [23]. Nevertheless, we do acknowledge the fact that K’s autistic traits are more visible in the classroom as he is in an environment that is most comfortable to him and the fact that he probably noticed that he was being observed. Hence, a more accurate observation would be for the camera to be hidden from view.
Another point of suggestion is to relate the child’s responses in HRI to his IQ level. K’s IQ level (non-verbal, verbal and full-scale) falls under the average to above average category. Thus, it is suggested that children with ASD in the same IQ group will be receptive to robot-based intervention even during the first child-robot session.
To wrap up, the overall comparison between observations during child-robot interaction and normal class setting in this particular case study supports our hypothesis that the humanoid robot NAO serves as a significant platform to support and initiate interaction in children with ASD. In the future, repeated exposure to the same robot in a longitudinal study is hoped to be able to train these children in interaction skills that are the constructive basis in building social and communication skills amongst the children with ASD. The need of long-term studies of HRI with children with ASD is undeniable however the duration and timing of the robotic exposure is crucial as not to create ‘permanent attachment’ and the preference of robotic contact compared to actual humans. These are some of the issues that we wish to embark upon at the next juncture of our study. We also plan to include more children with ASD to participate in our research in the future.
Acknowledgements
The authors gratefully acknowledge the Ministry of Higher Education Malaysia (MOHE), Universiti Teknikal Malaysia Melaka (UTeM), Universiti Teknologi MARA (UiTM) Shah Alam, Selangor and The National Autism Society of Malaysia (NASOM) for their support. A part of this project is supported by the Ministry of Higher Education Malaysia (MOHE) under the Fundamental Research Grant Scheme (FRGS) (600-RMI/FRGS 5/3/Fst/ (31/2011)).
References
- Buhler, "Robotics for rehabilitation--A European (?) perspective," Robotica, vol. 16, pp. 487-490, 1998.
- Feil-Seifer, "Socially Assistive Robot-Based Intervention for Children with Autism Spectrum Disorder," in IEEE International Conference on Robotics and Automation Workshop on Unifying Characteristics of Research in Human-Robot Interaction, Pasadena, CA, 2008, pp. pp. 10-11.
- J. Matarić, "Socially assistive robotics," IEEE Intelligent Systems, vol. 21, pp. 81-83, 2006.
- Boccanfuso and J. M. O’Kane, "CHARLIE: An Adaptive Robot Design with Hand and Face Tracking for Use in Autism Therapy," International Journal of Social Robotics, pp. 1-11, 2011.
- J. Diehl, L. M. Schmitt, M. Villano, and C. R. Crowell, "The clinical use of robots for individuals with Autism Spectrum Disorders: A critical review," Research in Autism Spectrum Disorders, 2011.
- P. Association and A. P. A. T. F. o. DSM-IV., Diagnostic and statistical manual of mental disorders: DSM-IV-TR: American Psychiatric Publishing, Inc., 2000.
- Kanner, "Autistic disturbances of affective contact," Nervous child, vol. 2, pp. 217-250, 1943. [8] L. Wing, "Autistic spectrum disorders," BMJ, vol. 312, pp. 327-328, 1996-02-10 00:00:00 1996.
- D. Kogan, S. J. Blumberg, L. A. Schieve, C. A. Boyle, J. M. Perrin, R. M. Ghandour, G. K. Singh, B. B. Strickland, E. Trevathan, and P. C. van Dyck, "Prevalence of parent-reported diagnosis of autism spectrum disorder among children in the US, 2007," Pediatrics, vol. 124, pp. 1395-1403, 2009.
- (2012, 29 April 2012). What is Autism. Available: http://www.nasom.com.my
- Bekele, U. Lahiri, J. Davidson, Z. Warren, and N. Sarkar, "Development of a novel robot-mediated adaptive response system for joint attention task for children with autism," in RO-MAN, 2011 IEEE, 2011, pp. 276-281.
- J. Dover and A. Le Couteur, "How to diagnose autism," Archives of disease in childhood, vol. 92, pp. 540-545, 2007.
- Weir and R. Emanuel, Using LOGO to catalyse communication in an autistic child: Department of Artificial Intelligence, University of Edinburgh, 1976.
- Michaud and C. Théberge-Turmel, "Mobile Robotic Toys and Autism," in Socially Intelligent Agents. vol. 3, K. Dautenhahn, A. Bond, L. Cañamero, and B. Edmonds, Eds., ed: Springer US, 2002, pp. 125-132.
- Adams and P. Robinson, "An android head for social-emotional intervention for children with autism spectrum conditions," Affective Computing and Intelligent Interaction, pp. 183-190, 2011.
- Kozima, C. Nakagawa, and Y. Yasuda, "Interactive robots for communication-care: A case-study in autism therapy," 2005, pp. 341-346.
- Costa, C. Santos, F. Soares, M. Ferreira, and F. Moreira, "Promoting interaction amongst autistic adolescents using robots," 2010, pp. 3856-3859.
- Dickstein-Fischer, E. Alexander, X. Yan, H. Su, K. Harrington, and G. S. Fischer, "An affordable compact humanoid robot for autism spectrum disorder interventions in children," 2011, pp. 5319-5322. M. Villano, C. R. Crowell, K. Wier, K. Tang, B. Thomas, N. Shea, L. M. Schmitt, and J. J. Diehl, "DOMER: a wizard of oz interface for using interactive robots to scaffold social skills for children with autism spectrum disorders," 2011, pp. 279-280.
- Scassellati, "Quantitative metrics of social response for autism diagnosis," 2005, pp. 585-590.
- J. Matarić, The robotics primer: Mit Pr, 2007.
- Akhtaruzzaman and A. Shafie, "Evolution of Humanoid Robot and contribution of various countries in advancing the research and development of the platform," 2010, pp. 1021-1028.
- J. Ricks and M. B. Colton, "Trends and considerations in robot-assisted autism therapy," 2010, pp. 4354-4359.
- Ranatunga, J. Rajruangrabin, D. O. Popa, and F. Makedon, "Enhanced therapeutic interactivity using social robot Zeno," 2011, p. 57.
- Robins, K. Dautenhahn, and P. Dickerson, "From Isolation to Communication: A Case Study Evaluation of Robot Assisted Play for Children with Autism with a Minimally Expressive Humanoid Robot," in Advances in Computer-Human Interactions, 2009. ACHI '09. Second International Conferences on, 2009, pp. 205-211.
- Robins, K. Dautenhahn, R. t. Boekhorst, and A. Billard, "Effects of repeated exposure to a humanoid robot on children with autism " in Cambridge Worshop Universal Access and Assistive Technology (CWUAAT), Cambridge, UK, 2004, pp. 225-236.
- Shamsuddin, L. I. Ismail, H. Yussof, N. Ismarrubie Zahari, S. Bahari, H. Hashim, and A. Jaffar, "Humanoid robot NAO: Review of control and motion exploration," in Control System, Computing and Engineering (ICCSCE), 2011 IEEE International Conference on, 2011, pp. 511-516.
- Gillesen, S. Boere, and E. Barakova, "WikiTherapist," in Proceedings of the 28th Annual European Conference on Cognitive Ergonomics, New York, USA, 2010, pp. 373-374.
- S. Erden and A. Tapus, "Postural expressions of emotions in a humanoid robot for assistive applications," 2010.
- Carey and J. Markoff, "Students, meet your new teacher, Mr. Robot," The New York Times, 2010.
- Giullian, D. Ricks, A. Atherton, M. Colton, M. Goodrich, and B. Brinton, "Detailed requirements for robots in autism therapy," 2010, pp. 2595- 2602.
- Shamsuddin, H. Yussof, L. Ismail, F. A. Hanapiah, S. Mohamed, H. A. Piah, and N. I. Zahari, "Initial response of autistic children in human-robot interaction therapy with humanoid robot NAO," in Signal Processing and its Applications (CSPA), 2012 IEEE 8th International Colloquium on , 2012, pp. 188-193.
- K. Morris. (2008, 10th June 2012). High-functioning autism. Available: http://www.autism-help.org/autism-high-functioning-hfa.htmAvailable: http://www.uvm.edu/
© 2012 The Authors. Published by Elsevier Ltd. Selection and/or peer-review under responsibility of the Centre of Humanoid Robots and Bio-Sensor (HuRoBs), Faculty of Mechanical Engineering, Universiti Teknologi MARA. Open access under CC BY-NC-ND license.
Ready to get started with your robot? click below to get get a free estimate, without any commitment"





 Too much to read? Don't have time?
Too much to read? Don't have time? 

.webp?width=124&height=124&name=image%20(1).webp)
.webp?width=169&height=87&name=image%20(2).webp)









